


The curious case of South Australian data
What the ☹ happened in 2021?

The Curious Case of South Australian Data – What the ☹ happened in 2021?
Data from South Australia makes a curious case. Why? Of significance, and unique to South Australia (SA), is that prior to the border opening on November 23 2021, SA had only had 922(1) cases of SARS-CoV-2/Covid-19 (herein Covid-19) since the start of the pandemic. As such, there was minimal to no Covid-19 in the state for most of 2021 (and 2020). However, in 2021 in SA there was an increasing Covid-19 vaccination rate with 88% of the SA population over the age of 15 “fully vaccinated” with 2 doses by the end of 2021. This creates ability for comparison of data between “pre-Covid” (2019, 2020), “pre-Covid but high vaccination” (2021), and “high Covid with high prior vaccination and boosters” (2022). It is noted that there were then 10,157 cases of Covid-19 reported from the time of the border opening on November 23 to the December 31 2021 SA Health report(2). As such, for the majority of 2021 South Australia had a highly vaccinated population with little to no Covid-19 in the state.
In late 2022, an FOI (FOI2022-00084) was submitted to the Department of Health and Wellbeing in SA requesting:
· Emergency Department (ED) Presentations and Hospital Inpatient (IP) admissions
· Selected ICD (disease diagnosis) codes (focussing on neurological and cardiac codes)
· ICD codes as Primary Diagnosis only
· Data to be presented monthly for the time period of Jan 1 2019 to Oct 31 2022.
After an internal review request, followed by an external review request to the SA Ombudsman, the data-set was finally released.
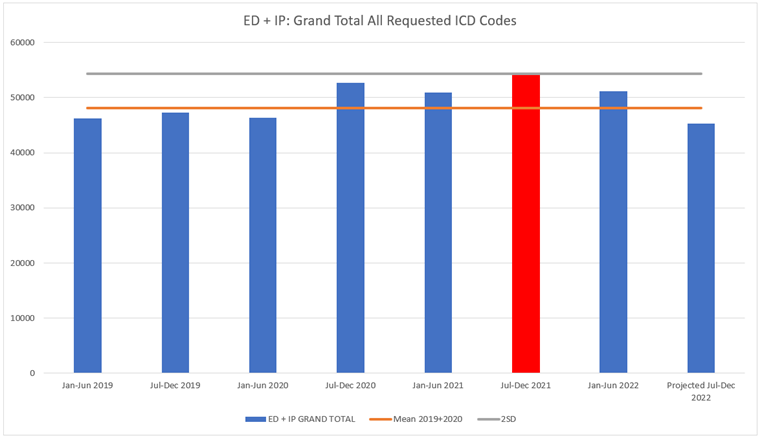
Data was initially reviewed per month for all combined ICD codes requested/provided as represented in Figure 1. The Mean was calculated based on the 2019 and 2020 data (Mean 2019+2020) to represent a pre-Covid-19 monthly average/usual number of combined ED+IP Presentations/Admissions per month for the requested/provided ICD codes. A clear increase is noted in 2021 as well as a peak in early 2022 coinciding with the 2021 Covid-19 vaccine rollout and booster doses. To reiterate, South Australia only had 922 cases of Covid-19 before Nov 24 2021 meaning the 2021 increase cannot be Covid illness related, whereas 88% of the SA population over the age of 15 were “fully vaccinated” with 2 doses by the end of 2021. To determine the relevance of this increase in 2021, a Fishers exact test was completed incorporating the population in SA from the Australian Bureau of Statistics latest state and territory population release. The test compared the count of the ICD codes of interest from Jan 2019 to Dec 2020 with Jan 2021 to Dec 2021. For all ICD codes requested/provided combined, the increase in ED and IP Presentations/Admissions in 2021 was found to be statistically significant (p<0.0001).
Figure 1: ED Presentations & Hospital Inpatient (IP) Admissions combined for all ICD Codes requested/provided combined per month, Jan 2019 to Oct 2022

To analyse the data further, monthly figures were pooled into 6-month blocks within calendar years. Data from 2019 and 2020 6-month blocks were used to calculate a Mean (average) and Standard Deviation (SD) to represent the usual 6-monthly number of ED Presentations plus Inpatient (IP) Hospital Admissions as well as the usual 6-monthly variance. As per Figure 2, the ED+IP data demonstrates a 2SD increase in the July to December 2021 6-month block – which for ED data alone was a 33% increase. As data was only provided for 4 months of Jul-Dec 2022, the 4 months provided was divided by 4 to reach a monthly usual amount which was then multiplied by 2 to then add to the provided 4 months to create a projected 6-month block for all ICD codes combined in order to determine the overall likely trend in 2022.
Figure 2: ED Presentations & Hospital Inpatient (IP) Admissions per 6-month block all provided ICD codes combined
To review contributing disease diagnoses, related ICD codes were grouped and reviewed again monthly and per 6-month blocks, and again compared to a Mean from 2019 and 2020 data, and the Fishers exact test was completed in the same manner previously described. ED Presentations plus Hospital IP Admissions for Encephalitis, Encephalopathy, Myelitis, Transverse Myelitis, Bells Palsy, Polyneuropathies, and Guillain Barre Syndrome (GBS) combined in 2021 demonstrated a statistically significant increase (p<0.0001) compared to 2019 and 2020 (Figure 3). Both the ED and IP data were affected by the increase.
Figure 3: ED Presentations plus Hospital Inpatient (IP) Admissions for Encephalitis, Encephalopathy, Myelitis, Transverse Myelitis, Bells Palsy, Polyneuropathies, and GBS

Comparing the 6-month blocks for pooled data for Encephalitis, Encephalopathy, Myelitis, Transverse Myelitis, Bells Palsy, Polyneuropathies, and GBS, both the Jan-Jun 2021 and July-Dec 2021 6-month blocks likely contributed to the statistically significant increase (Figure 4) having a 2 and 3 SD increase respectively, with the July-Dec 2021 data being a 15.8% increase from the Mean.
Figure 4: ED and IP Presentations/Admissions for Encephalitis, Encephalopathy, Myelitis, Transverse Myelitis, Bells Palsy, Polyneuropathies, and GBS, per 6-months

Ischaemic Heart Disease (IHD) also showed a statistically significant increase (p<0.0001) in 2021 compared to 2019 and 2020 for ED Presentations and Hospital IP Admissions combined (Figure 5).
Figure 5: ED and IP Presentations/Admissions for Ischaemic Heart Disease (IHD) per month

Comparing the 6-month blocks for IHD ED Presentations plus Hospital Admissions, both the Jan-Jun 2021 and Jul-Dec 2021 6-month blocks likely contributed to the statistically significant increase having more than a 2 and 5 SD increase respectively, which is a 50.6% increase for the July-Dec 2021 6-month block (Figure 6) .
Figure 6: ED plus IP Presentations/Admissions for Ischaemic Heart Disease (IHD) per 6-month block

Monthly data for ED Presentations plus Hospital IP Admissions for Pericarditis also showed a statistically significant increase (p=0.0008) in 2021 compared to 2019 and 2020 (Figure 7) with both ED and IP data impacted.
Figure 7: ED plus IP Presentations/Admissions for Pericarditis per month

For ED Presentations combined with Hospital IP Admissions for Pericarditis only the Jul-Dec 2021 6-month block appears to have contributed to the statistically significant increase in 2021 with an increase of more than 3 Standard Deviations, or a 46% increase (Figure 8). Noting the 2022 data remains high.
Figure 8: ED plus IP Presentations/Admissions for Pericarditis per 6-month block

Monthly data for ED Presentations plus Hospital IP Admissions for Myocarditis in 2021 also showed a statistically significant increase (p<0.0001) compared to 2019 and 2020 (Figure 9) with both ED and IP data impacted.
Figure 9: ED plus IP Presentations/Admissions for Myocarditis per month

For myocarditis both 6-month blocks of 2021 demonstrate a possible contribution toward the statistically significant increase in 2021, whereby Jul-Dec is a 17 Standard Deviation or 202% increase from the 2019+2020 Mean (Figure 10).
Figure 10: ED plus IP Presentations/Admissions for Myocarditis per 6-month block

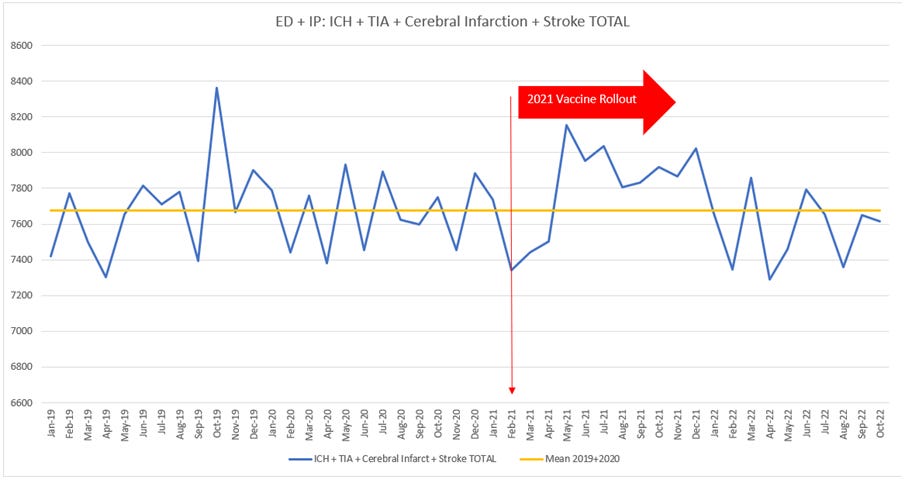
Monthly data for stroke type events (ICH: Intracerebral Haemorrhage, TIA: Transient Ischaemic Attack, Cerebral Infarction and Stroke combined) demonstrated a statistically significant increase (p=0.0256) compared to 2019 and 2020 (Figure 11) with both ED and IP data impacted.
Figure 11: ED plus IP Presentations for Stroke Type events per month
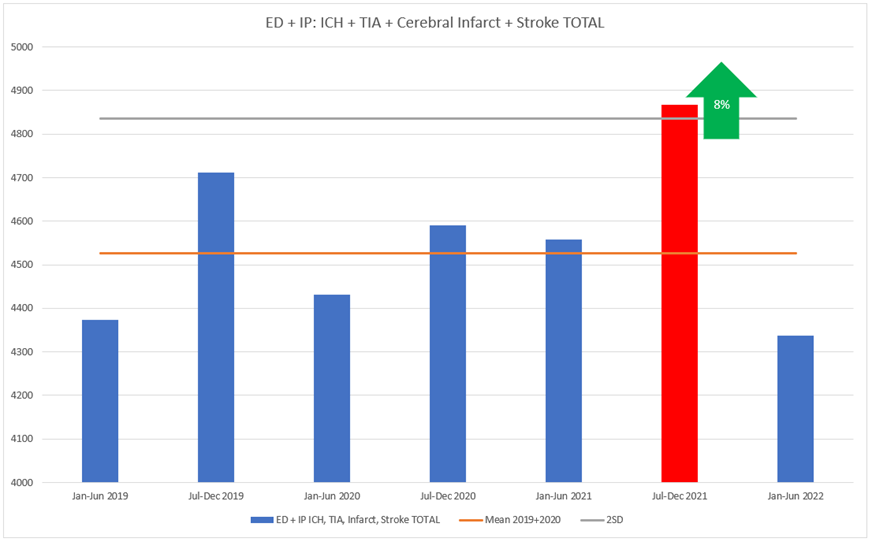
ED Presentations plus Hospital IP Admissions for the Jul-Dec 2021 6-month block for stroke type events demonstrates a likely contribution to the statistically significant increase, noted as an 8% increase from the 2019+2020 Mean (Figure 12).
Figure 12: ED plus IP Presentations/Admissions for Stroke Type events per 6-month block
ED Presentations plus Hospital IP Admissions for Abnormalities of Heart Beat also demonstrate a statistically significant increase (p<0.0001) compared to 2019 and 2020 (Figure 13).
Figure 13: ED plus IP Presentations/Admissions for Heart Beat Abnormalities for month

While the combined ED plus IP data for Abnormalities of Heart Beat did not reach a 2 SD increase in either 6-month block in 2021 (Figure 14), the ED data alone did reach a 2 SD increase in the July-Dec 2021 block (Figure 15). Noting that Jan-Jun 2022 has also reached a 2SD increase.
Figure 14: ED plus IP Abnormalities of Heart Beat per month (left) and
Figure 15: ED only Abnormalities of Heart Beat per month (right)

The ED plus IP Presentations/Admissions per month for Chest Pain also showed a statistically significant increase (p<0.0001) compared to 2019 and 2020 (Figure 16), with ED data predominantly impacted.
Figure 16: ED plus IP Presentations/Admissions for Chest Pain per month

Both the Jan-Jun 2021 and Jul-Dec 2021 6-month blocks for ED plus IP Presentations/Admissions for Chest Pain contributed to the statistically significant increase in 2021, noting the Jul-Dec 6-month block is a 6 Standard Deviation or 16% increase from the 2019+2020 Mean (Figure 17), and the 2022 data remains increased. For ED data alone, the increase in the Jul-Dec 2021 6-month block for Chest Pain is a 29% increase from the 2019+2020 Mean, which is an additional 650 ED Presentations per month (around 22 more per day) and nearly 4000 potential people affected compared to usual over 6 months. Why is there such an increase in numbers of Chest Pain, particularly in ED versus admitted? Were people being turned away, or discharged without further investigation or diagnosis?
Figure 17: ED plus IP Presentations/Admissions for Chest Pain per 6-months

Data was only present for ED for Systemic Inflammatory Response Syndrome (SIRS) which showed a statistically significant increase (p<0.0001) compared to 2019 and 2020 (Figure 18).
Figure 18: ED only for Systemic Inflammatory Response Syndrome (SIRS) per month

The ED only data for Systemic Inflammatory Response Syndrome (SIRS) showed more than a 2 Standard Deviation increase in the Jul-Dec 2021 6-month block as likely contributing to the statistically significant increase for 2021 that has continued to increase into 2022 (Figure 19).
Figure 19: ED only for Systemic Inflammatory Response Syndrome (SIRS) per 6-month block

Of interest there was also a statistically significant increase (p<0.0001) in Unknown and Unspecified Cause of Morbidity for ED plus IP Presentations/Admissions data per month (Figure 20).
Figure 20: ED plus IP Presentations/Admissions for Unknown and Unspecified Cause of Morbidity per month

However, the 6-month block data analysis for Unknown and Unspecified Cause of Morbidity did not quite reach 2 Standard Deviation in the Jul-Dec 2021 6-month block (Figure 21).
Figure 21: ED plus IP Presentations/Admissions for Unknown and Unspecified Cause of Morbidity per 6-month block

The knowledge of the increase in SA’s Cardiac related data is however, not new, given Senator Antic’s FOI(3) that was dismissed as NOTHING to SEE HERE by The Advertiser and SA Health’s Chief Primary Health Officer Professor Nicola Spurrier(4). What this does show us however, is that Prof Nicola Spurrier, SA Health and therefore no doubt Premier Malinauskas and the Minster for Health, Chris Picton, are AWARE of such increased data-sets. And yet, they don’t seem concerned enough to do anything about it, or consider it a problem, let alone associate it with the vaccine. This is despite the fact that once again there was essentially NO Covid-19 in the state in 2021, but there was an increasing vaccination rate.

We have also all been told about myocarditis as a risk factor and that it is supposedly mild and recoverable - never mind the possible long-term implications of cardiomyopathy…. Or the fact that people have died from myocarditis associated with the Covid-19 vaccines… Or that the ATAGI Guidance on Myocarditis and Pericarditis after COVID-19 vaccines document(5) states that months after mRNA Covid-19 vaccine associated myocarditis, follow-up cardiac MRI studies show the persistence of late gadolinium enhancement in areas of people’s myocardium, which can be evidence of myocardial scarring. What they don’t state is that myocardial scarring can lead to ongoing cardiac dysfunction, cardiomyopathy, and pre-mature morbidity or death….

But what about the neurological data, is the stroke data unexpected?….
Not really…. I mean firstly, medically speaking, it is also a vascular event. But also, it is not unexpected when you consider that there were a large number (300 events in 275 people) of strokes reported to Pfizer in the first 90 days of the post market surveillance of which 1 in 5 died(6). Of note, the SA Health data above represents people with a stroke that survived….enough so at least present to hospital or be admitted…. But furthermore, according to the Therapeutic Goods Administration (TGA) DAENs database the increase in stroke admissions is also not surprising…. Whilst the data is “conveniently” spread across a large number of stroke-related MedDRA’s there is at least 1166 stroke-related events reported (noting this may be significantly under-reported and may not represent all stroke-related fields) through to Jan 4th 2023, with 138 of these having death as an outcome (Figure 22).
Figure 22: TGA DEANs Stroke-related MedDRA Jan 1 2021 to 4 Jan 2023

Source: · DAEN Portal (tga.gov.au) https://daen.tga.gov.au/medicines-search/
In fact, if we look at All Nervous System Disorders Top 25 (Figure 23) from the TGA DAENs database many of the conditions appearing in the SA Health data above also appear in the Top 25 Nervous Systems Disorders list….. That is, diagnoses in the top 25 neurological symptoms being reported to the TGA directly about the Covid-19 vaccines also appear as the diagnoses with increased numbers of ED Presentations and IP Admissions in the SA Health data in 2021 where there was essentially no Covid-19 and a high vaccination rate…. Coincidence?..............
Figure 23: TGA DAENs database Top 25 All Nervous System Disorders

Just to be clear about the fact that SA essentially had no Covid-19 in the state but high vaccination rates: As per the table below, which was last updated on 5th December 2022, South Australia achieved a 91.8% 2-dose vaccination rate and a 76.2% 3-dose vaccination rate of people eligible for 3 doses.
Vaccine coverage by jurisdiction - people aged 16 and over

Source: Vaccination numbers and statistics | Australian Government Department of Health and Aged Care / https://www.health.gov.au/our-work/covid-19-vaccines/vaccination-numbers-and-statistics#jurisdictional-data Last Updated 5 Dec 2022
However, the VAST majority of Covid-19 vaccination for 2 doses occurred in South Australia in 2021 as indicated in the Geographic Vaccination Rates table below.

Source: COVID-19 vaccination – Geographic vaccination rates – SA4 – 4 January 2021 (health.gov.au) https://www.health.gov.au/sites/default/files/documents/2022/01/covid-19-vaccination-geographic-vaccination-rates-sa4-4-january-2021.pdf Full list COVID-19 vaccination – Geographic vaccination rates – SA4 | Australian Government Department of Health and Aged Care
And the VAST majority of boosters were given in South Australia by the end of February 2022 with notably less uptake of the 3rd dose (and then particularly of the 4th dose….).

Source: SA4 - Geographic Vaccination Rates (health.gov.au) https://www.health.gov.au/sites/default/files/documents/2022/02/covid-19-vaccination-geographic-vaccination-rates-sa4-28-february-2022.pdf
Graphically, for all of Australia (with SA being similar) this can be represented as below.

Source: Coronavirus (COVID-19) Vaccinations - Our World in Data https://ourworldindata.org/covid-vaccinations?country=~AUS
Is any of this unexpected…. Not when you consider there is over 1250 articles(7) on adverse events including the very cardiac and neurological events discussed within. So, while correlation may not equal causation, there is scientific literature supporting the Covid-19 vaccines as the cause for all of these conditions presenting to SA Health hospitals. One question to consider is whether the increases in ED Presentations and IP Admissions in the Jun-Dec 2021 data could be caused by the 10,000+ Covid-19 cases in the state after the borders were opened, so from Nov 24 2021 to December 2021? The answer is no, that has been checked…. December data was not increased comparative to Jul, Aug, Sept, Oct or Nov 2021, and Figure 1 also demonstrates no increase in ED Presentations plus Hospital IP Admissions for the December 2021 or June/July 2022 Covid-19 waves that SA had. So once again, it simply was not a sudden exposure to Covid-19 that caused the statistically significant increases in the SA Health data demonstrated – in fact the ED and IP data for SA is at it its lowest or on the way down, when Covid-19 was at its greatest in the state as per Figure 1. So, Professor Spurrier, something else in 2021 and early 2022 had to have caused this. And in any case, the fact that the data for 2022 overall returns to normal (Figure 1), as well as returns to normal for a range of conditions in the 6-month blocks, does not support the hypothesis that the virus is causing much of these issues at all. It is more likely that booster doses are contributing, especially as younger age groups were made eligible to receive the vaccination over time.
Well, that alone would all seem pretty bad, right….. I mean besides the personal impact on individuals and families of all these increased ED Presentations and Hospital Admissions from probable vaccine injuries (which is the real tragedy here), wouldn’t this also have a negative impact on the capacity of the SA Healthcare system including ramping(8) ….. Isn’t ramping (ironically) the one thing Premier Peter Malinauskas so desperately wants to fix in SA as his election promise(9) and his need to ‘save political face on this one’… and after all, didn’t he state he is very aware of the personal impact of ramping(10) and the potentially preventable tragedy of a 47-year-old father dying following a heart attack while waiting for an ambulance in SA(11). Wouldn’t therefore Premier Malinauskas be very concerned to hear about this data and be keen to get to the bottom of it…. One would think so.
Considering ramping, what exactly was the impact on the SA Ambulance System? Using the annual reports for 2017-2018, 2018-2019, 2019-2020 and 2020-2021 (2021-2022 not yet available) there was in 2020-2021 on average 108 more triple zero calls per day than the mean per day of the 3 prior financial years and on average 71 more triple zero call per day in 2020-2021 than 2019-2020 (Table 1), noting the difference between previous financial years was only an increase of 39 and 36 daily calls for 2018-2019 and 2019-2020 respectively.
Table 1: Daily Average Triple Zero Calls Received and Incidents Responded To by SA Ambulance per Financial Year

Looking at the total number of triple zero calls answered per financial year, the 2020-2021 financial year saw a whopping 10.6% increase (25,866 additional calls) to the prior financial year, compared to only a 6.37% mean increase for the prior 3 financial years (Figure 24). This is tens of thousands more calls when there was only 922 Covid-19 cases in the state for 2019 and 2020 combined. Using the same analysis approach as for the ICD codes above, this is a nearly 3 SD increase from the mean of the prior years and is once again statistically significant.
Figure 24: Total Triple Zero Calls to SA Ambulance per Financial Year

The data from the SA Health hospitals and the SA Ambulance annual reports presented above is consistent with that reported by the Australian Institute of Health and Welfare(12) (AIHW) in their Emergency department care 2021-22 data tables: Table 2.2 Emergency department presentations, by state and territory, 2017-18 to 2021-22. The AIHW data shows that in the 2020-2021 Financial year SA had a whopping increase of 45,122 ED presentations to the year prior, while for the two previous financial years the change from the prior year was only 13,113 and 15,846 for the 2018-19 and 2019-20 years respectively. Further, in the 2021-2022 financial year there is a decrease of 1.3% in ED presentations reported by the AIHW with an average change of 3.1% reported since 2017-18 but the change in 2021-2022 to the prior year is 8.4%….
Did someone also forget to tell the AIHW that SA only had 922 cases of Covid-19 for all of 2020 and 2021 combined? Given that, what caused the 45,122 extra ED Presentations in the 2020-2021 financial year, if it wasn’t Covid-19?
The data in Table 2.2 from the AIHW is also reported as a per 1,000 population which consistent with the total data shows an unusually large increase of 24.6 ED presentations more per 1000 to the year prior and then again a decrease in the 2021-2022 data…

The AIHW Website(13) will even provide their own graph of this for you.

At least to minimise the impact on ramping there were lots of healthcare staff ready and available to assist…. Right?
All hands were on deck, right?
Wrong…..
In another FOI relating to Covid-19 sick leave amongst SA Health staff it was found that sick leave hours increased by 7.5% in 2021 (p=0.03) and 47% (p<0.001) in 2022 with both Covid-19 and non-Covid reasons represented for 2022 (Figure 25). From this, it seems the SA Health staff were also more sick from non-Covid-19 reasons in 2022…..
Furthermore, from the same FOI, 15,500 vaccinated SA Health staff (approx. 40%) were noted to have caught Covid-19 (been on sick leave with Covid-19) in the first 9 months of 2022 (data unavailable for 2021) despite being 2-dose vaccinated by the November 1 2021 mandate and 3-dose vaccinated by the Jan 29 2022 mandate. This resulted in 447,793 Hours of sick leave across 15,550 SA Health employees which equates to an average of 218 shifts per day (assuming 7.5H shifts and continued service across 24H) for the 273 days of Jan to Sept 2022. Of course, this would vary pending admin versus clinical roles, day shifts to night, and is varied month to month according to the Covid-19 waves in the state. AND, on top of this, unvaccinated staff were not allowed, and are still not allowed, to work, despite a large number of vaccinated SA Health staff catching Covid-19 and Covid-19 vaccines not impacting transmission .… adding overall to a complete disaster of short staffing and further deceased capacity of the healthcare system and hospital staff to assist with the flow through of patients to reduce ramping.
Figure 25: SA Health Sick Leave Hours

Image credit: Arkmedic
In fact in one week in July 2022, over 1200 triple-vaccinated SA Health staff were off work with Covid-19 and at a similar time so were over 80 triple-vaccinated SA Ambulance officers….. talk about a Health Care Crisis!!! Lucky no one died because of this….oh wait……………………………..


So, we have the perfect storm regarding impact on healthcare capacity of increased ED Presentations and Hospital IP Admissions contributed in part to likely vaccine related injuries in 2021, combined with and followed by, increased staff shortages from vaccinated staff catching Covid-19 and unvaccinated staff not being allowed to work – no wonder ramping has been so bad!
Ironically Premier Malinauskas, you have caused your own ramping crisis (in part at least) and people’s health has clearly been placed at risk.
And still, Premier Malinauskas, Minister for Health Chris Picton, Prof Nicola Spurrier and SA Health will NOT LET UNVACCINATED HEALTHCARE WORKERS RETURN TO WORK to assist in addressing this healthcare crisis, whereby they still claim an impact of the vaccines on transmission despite court rulings clearly stating that there is not(14).

In fact, the new SA Health vaccination policy(15), that has been implemented in late November 2022, and which mandates Covid-19 vaccination for all clinical staff as well as students, is based on reducing transmission. Further ironies relating to this Policy include, that influenza vaccination is only recommended not mandated, and the vaccinated SA Health staff have not been forced to be vaccinated since Jan 2022, yet SA Health acknowledge waning (which if anything is against symptomatic illness only….if that) to occur in 4 or less months following your last dose! So, SA Health and Prof Nicola Spurrier know their ‘vaccinated’ working staff have no more protection than any unvaccinated staff member who is not allowed to work. And they certainly won’t consider natural immunity…..

Image source: SA+Health+Policy+-+Occupational+assessment+screening+and+vaccination+-+20221118.pdf
Another question or response commonly heard is that “it could have been worse.… there might have been more cases in the SA Health staff if they were not vaccinated….”. Well, NO.
In a recent Cleveland Clinic study(16) the risk of Covid-19 infection increased with the increased number of doses of Covid-19 vaccine (Figure 26). That is the more doses you have, the more likely you are to be infected with Covid-19. In this study, people who had received three or more injections were more than 3x as likely to be infected as those that had received none. So, force vaccinating all of the SA Health and SA Ambulance workers most likely increased the number of Covid-19 cases amongst them (let alone the general population…).
Well done Premier Malinauskas, Prof Nicola Spurrier, the Hon Chris Picton and SA Health, way to protect those vulnerable patients…
Figure 26: Image from Cleveland Clinic study showing increased cases with increased doses

This information however, is not that new, with this study(17): “Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study” demonstrating that after 3 months, Pfizer jab recipients are 76.5% more likely than unvaccinated individuals to contract the Omicron variant. This again indicates that the vaccines are leading to an increased risk of cases/infection, and once infected therefore increased transmission.
Further, in another study(18): “Duration of Shedding of Culturable Virus in SARS-CoV-2 Omicron (BA.1) Infection” it was demonstrated that vaccinated individuals were sicker for a longer duration and therefore transmission and duration of transmission risk is increased with vaccination. In the study, triple vaccinated/boosted people recovered significantly more slowly from Covid-19 and remained contagious for much longer than unvaccinated people. Huh…
Again, the common response is… “but the risk of issues following Covid-19 infection still outweighs the risk of adverse events from vaccination”…. Well, firstly, that is a personal and individual choice on a case-by-case discussion with one’s own doctor and has nothing to do with transmission which is what has been used to justify mandates and the new SA Health Policy… But also, Well No, for most people that is not the case.
Using Myocarditis and Pericarditis as one example this large-scale Israeli study of 196,922 unvaccinated adults after Covid-19 infection showed that Covid-19 infection was not associated with myocarditis or pericarditis(19) So, it is simply not true that myocarditis is worse after Covid-19 infection as compared to myocarditis following vaccination (which it is associated with even according to the TGA and ATAGI who also acknowledge long term myocardial scarring potential….).
In another study(20) it was noted that Covid-19 boosters are likely to cause a net clinical harm to young adults (18-29yo) where total severe adverse events outweigh Covid-19 hospitalisations.
The risk/harms from Covid-19 vaccines have also been demonstrated to outweigh the risk/harms for catching Covid-19 as indicated in this study: “Serious Adverse Events of Special Interest Following mRNA Vaccination in Randomized Trials”(21) where a 1 in 800 risk of serious adverse events post Covid-19 vaccination is reported. Furthermore, in this study, the excess risk of serious adverse events of special interest surpassed the risk reduction for Covid-19 hospitalisation relative to the placebo group in both Pfizer and Moderna trials (2.3 and 6.4 per 10,000 participants, respectively) meaning the greater risk is to the vaccinated.
And yet another study: “Curing the pandemic of misinformation on COVID-19 mRNA vaccines through real evidence-based medicine - Part 1”(22) also demonstrates a greater risk of serious adverse events from the vaccines than being hospitalised from Covid-19 infection and that the number needed to treat in the non-elderly population to prevent a single death runs into the thousands.
Simply put, what this research shows is that the risk of harm from taking the Covid-19 vaccines outweighs the risk of harm from catching Covid-19.
To further clarify that the Covid-19 vaccines do not have a positive result on severity, reducing hospital admissions, and deaths, this study: “Increasing SARS-CoV2 cases, hospitalizations and deaths among the vaccinated elderly populations during the Omicron (B.1.1.529) variant surge in UK”(23) found a significantly increased proportion of Covid-19 cases, hospitalisation and deaths amongst the vaccinated for the Omicron variant along with significantly decreased cases, hospitalisations and deaths for the unvaccinated.
Still not convinced…..
Well, our Australian data from NSW (SA does not have good data to access… not easily anyway…) aligns with the article above where there appears to be a dose dependent increased hospitalisation, ICU and Death rate per 1M amongst the vaccinated (Figure 27).
Figure 27: NSW Health Surveillance Data Hospitalisation/ICU/Death per 1M by Vaccination Status
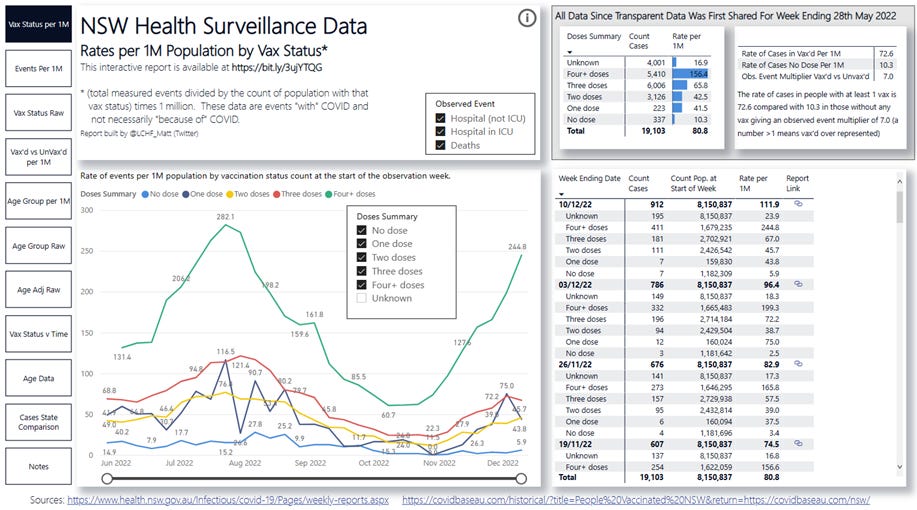
Source: https://bit.ly/3ujYTQG and credit to the creator of this interactive site
Furthermore, the last NSW Surveillance Report(24) (dated ending 31 Dec 2022) that NSW Health will include the breakdown of hospital admissions, ICU admissions and deaths by vaccination status (Figure 28), clearly shows that if severity was measured by admissions to hospital and ICU or death that the vast majority presently occur in vaccinated patients.
Figure 28: Admissions to Hospital, ICU and deaths for fortnight ending 31 Dec 2022 NSW

In yet another FOI to SA Health, they did have to give up some data (Figure 29) similar to the NSW reports. What this showed was a mere 8% of those hospitalised in SA “for” Covid-19 from 1/1/21 to 27/6/2022 were unvaccinated, which aligns with what the NSW data has been telling us…. So why are we still hearing from Prof Nicola Spurrier and SA Health that the Covid-19 vaccinations reduce severe illness and hospitalisation(25), when this is their own data?
Figure 29: Numbers of People Admitted to Hospital for Covid-19 in South Australia by Vaccination Status

So, you think this would all be of great concern to Premier Malinauskas…. I mean even if he only cares about ramping (for his own Political gain)…. You would also think he would know, or would want to know….
Yet, when asked in a conversation with Premier Malinauskas about all of this, he insisted the vaccines reduce transmission….
He stated that he takes a philosophical approach and needed the unvaccinated healthcare workers allowed back at work to FIX RAMPING - aka to make him look good on his political promise - not to help the SA Public with their health care needs or support the current workers who are under constant pressure with daily Code White’s (capacity emergency)…. Yet when asked what he would therefore do about this, his response was that he has nothing to do with SA Health….
And, he stated that all of this information (which has been sent, plus much much more, to his office – and to Prof Spurrier – and to SA Health - yet he was seemingly unaware of it…) is simply in the scientific minority…. I wonder, how many articles from how many different independent scientists, doctors and researches needs to be sent to him, Prof Spurrier, SA Health and the Hon Chris Picton? It has been a good 20+ pages of references so far…… So that begs the question, is it ignorance, negligence, intent or malfeasance?
And well Premier Malinauskas…. What about our OWN DATA? Why are you not concerned about that? Why did Prof Nicola Spurrier dismiss the cardiac data, that you would also therefore know about and would impact ramping? After all, it is only the people of South Australia’s lives and health of concern…. Right?
References
1 COVID-19 update 1 December 2021 | SA Health https://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/about+us/news+and+media/all+media+releases/covid-19+update+1+december+2021
2 COVID-19 update 31 December 2021 | SA Health https://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/about+us/news+and+media/all+media+releases/covid-19+update+31+december+2021
6

7 1250+ COVID Vaccine Publications and Case Reports - React19 https://react19.org/1250-covid-vaccine-reports/
8 'Worst results on record': Ramping still rampant (indaily.com.au) https://indaily.com.au/news/2022/12/22/worst-results-on-record-ramping-still-rampant/
10 'These aren’t just news stories': Malinauskas predicts years-long ramping fix (indaily.com.au)
11 Adelaide man, 47, dies after waiting 40 minutes for ambulance to arrive - ABC News
12 Emergency department care - Australian Institute of Health and Welfare (aihw.gov.au) https://www.aihw.gov.au/reports-data/myhospitals/sectors/emergency-department-care
13 Emergency department care activity - Australian Institute of Health and Welfare (aihw.gov.au) https://www.aihw.gov.au/reports-data/myhospitals/intersection/activity/ed
14 2023-1-13-doc-86-decision-and-order.pdf (childrenshealthdefense.org)
15 SA+Health+Policy+-+Occupational+assessment+screening+and+vaccination+-+20221118.pdf https://www.sahealth.sa.gov.au/wps/wcm/connect/b65b12804f0cbdd29178b7791a12b24c/SA+Health+Policy+-+Occupational+assessment+screening+and+vaccination+-+20221118.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-b65b12804f0cbdd29178b7791a12b24c-ojAr9pc
16 Shrestha, N. K., Burke, P. C., Nowacki, A. S., Simon, J. F., Hagen, A., & Gordon, S. M. (2022). Effectiveness of the Coronavirus Disease 2019 (COVID-19) Bivalent Vaccine. medRxiv, 2022-12. https://doi.org/10.1101/2022.12.17.22283625
17 Hansen, C. H., Schelde, A. B., Moustsen-Helm, I. R., Emborg, H. D., Krause, T. G., Mølbak, K., & Valentiner-Branth, P. (2021). Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. MedRxiv, 2021-12. Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study | medRxiv https://doi.org/10.1101/2021.12.20.21267966
18 Boucau, J., Marino, C., Regan, J., Uddin, R., Choudhary, M. C., Flynn, J. P., ... & Barczak, A. K. (2022). Duration of shedding of culturable virus in SARS-CoV-2 Omicron (BA. 1) infection. New England Journal of Medicine, 387(3), 275-277. Duration of Shedding of Culturable Virus in SARS-CoV-2 Omicron (BA.1) Infection | NEJM DOI: 10.1056/NEJMc2202092
19 Tuvali, O., Tshori, S., Derazne, E., Hannuna, R. R., Afek, A., Haberman, D., ... & George, J. (2022). The Incidence of Myocarditis and Pericarditis in Post COVID-19 Unvaccinated Patients—A Large Population-Based Study. Journal of Clinical Medicine, 11(8), 2219. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9025013/ https://doi.org/10.3390/jcm11082219
20 Bardosh, K., Krug, A., Jamrozik, E., Lemmens, T., Keshavjee, S., Prasad, V., ... & Høeg, T. B. (2022). COVID-19 vaccine boosters for young adults: a risk benefit assessment and ethical analysis of mandate policies at universities. Journal of medical ethics. https://jme.bmj.com/content/early/2022/12/05/jme-2022-108449
21 Fraiman, J., Erviti, J., Jones, M., Greenland, S., Whelan, P., Kaplan, R. M., & Doshi, P. (2022). Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults. Vaccine, 40(40), 5798-5805. https://www.sciencedirect.com/science/article/pii/S0264410X22010283 https://doi.org/10.1016/j.vaccine.2022.08.036
22 Malhotra, A. (2022). Curing the pandemic of misinformation on COVID-19 mRNA vaccines through real evidence-based medicine-Part 1. Journal of Insulin Resistance, 5(1), 8. https://insulinresistance.org/index.php/jir/article/view/71 https://doi.org/10.4102/jir.v5i1.71
23 Emani, V. R., Pallipuram, V. K., Goswami, K. K., Maddula, K. R., Reddy, R., Nakka, A. S., ... & Goswami, S. (2022). Increasing SARS-CoV2 cases, hospitalizations, and deaths among the vaccinated populations during the Omicron (B. 1.1. 529) variant surge in UK. medRxiv, 2022-06. https://doi.org/10.1101/2022.06.28.22276926
24 https://www.health.nsw.gov.au/Infectious/covid-19/Documents/weekly-covid-overview-20221231.pdf
25 COVID-19 Vaccinations | SA Health https://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/conditions/infectious+diseases/covid-19/vaccine/covid-19+vaccinations
Thanks to the mice who helped in this process as one person alone could not have done this.
Are you interested in helping me share the QLD data?
https://thetenthman.substack.com/p/for-your-consideration-myocarditis
Cheers
Excellent! I hope politicians and public health authorities are starting to squirm and realizing we WILL be insisting upon trials. They all knew very early on that these experimental injections are very dangerous and yet they did NOTHING. Instead, the mandated them! Everything they did made the situation worse. NO AMNESTY. Too many people have died or been seriously injured for that. Thank you for digging up the evidence. Hang onto it!